key:article.publicationhighlight Man Jiang, Jikui Deng, Guanglun Zhou, Shoulin Li and Gang Liu, Pediatric Urology, 2022
This study by Jiang et al is one of the few studies focusing on the risk factors of recurrent UTIs in a large group of children with neurogenic bladder using intermittent catheterization (IC). The study consists of a comprehensive analysis of clinical and urodynamic indicators in children between 9 months and 12 years. Children with neurogenic bladders who experience recurrent UTIs have a high risk of developing severe kidney damage, hence the need for greater focus on this issue. This study is useful in determining treatments and proactive measures for preventing recurrent UTIs.
What is Neurogenic Bladder?
Neurogenic bladder (NB) means a dysfunction in the bladder capacity caused by a spinal cord lesion at any level. This condition contributes to issues like urine retention, incontinence, urinary tract infection (UTI) and vesicoureteral reflux (VUR). The urine will normally flow from the kidneys through the ureters down to the bladder. VUR is the abnormal flow of urine from the bladder back up the tubes (ureters) that connect the kidneys and bladder. Ultimately these problems may lead to renal scarring. Once the filters of the kidneys have been scarred, they cannot be repaired. If the scarring becomes significant enough, the damage can lead to severe kidney failure.
Treatment of Neurogenic Bladder
Immediately after the confirmed diagnosis of neurogenic bladder, treatment should be performed to avoid serious complications. Intermittent catheterization (IC) is usually the recommended therapy and first choice for bladder management to avoid complications. IC is shown to significantly decrease the risks of damage to the kidneys by reducing the bladder pressure and preventing upper urinary tract damage.
Recurrent UTIs in Children
Despite the many advantages of using IC for bladder management, it involves an increased risk of UTIs compared to normal voiding. Some patients with NB managed by IC have recurrent UTIs, causing a negative impact on quality of life and need for long periods of antibiotic treatments. Others will rarely or never experience recurrent UTIs. Hence, there may be certain risk factors increasing the risk of recurrent symptomatic (needed to be treated) UTIs. It’s of utmost importance to identify possible risk factors in children suffering from recurrent symptomatic UTIs, aiming for preventive strategies, and avoiding renal scarring and serious kidney failure.
Aim of Study and Set Up
The exact reasons for recurrent symptomatic UTIs are not fully understood. Opinions differ whether there is a direct relationship between urodynamic disorders and the incidence of recurrent UTIs, or if clinical factors are mainly responsible. This study aims to identify the clinical, demographic, and urodynamic risk factors associated with the incidence of recurrent symptomatic UTIs in children with NB. This was done by retrospectively reviewing the clinical information of 327 patients diagnosed with NB between 2014 to 2018 at the national Center for Children’s Health in Beijing. Ultrasonic and urodynamics parameters were collected in the beginning of the study period and all patients were followed for at least 1 year and had minimum two clinic visits during the study period. All data was compared between the recurrent UTI (>1.0 UTI/study-year) and episodic UTI (≤1.0 UTI/study-year) groups.
Treatment of UTIs in Children
The results showed that children with recurrent UTIs were more likely to have poor function of the kidneys and thereby the prevention of recurrent UTIs is vital. The study also revealed that children of older age were more likely to get recurrent UTIs. Also, the level of spinal cord injury and how long they suffered from neurogenic bladder had an impact. Vesicoureteral reflux (backflow of urine), bladder wall thickness (BWT) and bladder compliance were also shown to have a direct association with the cause of recurrent UTIs. Furthermore, they concluded that clinical and urodynamic characteristics of the urinary tract may worsen over time in children with NB and thereby it’s important to conduct long-term follow up. The authors recommend that patients with VUR, increased BWT, and low bladder compliance should be followed up once every 6 months to 1 year. They also showed that continuous antibiotic prophylaxis is not recommended for the prevention of UTIs in patients with NB.
Causes of UTIs in Children with Neurogenic Bladder
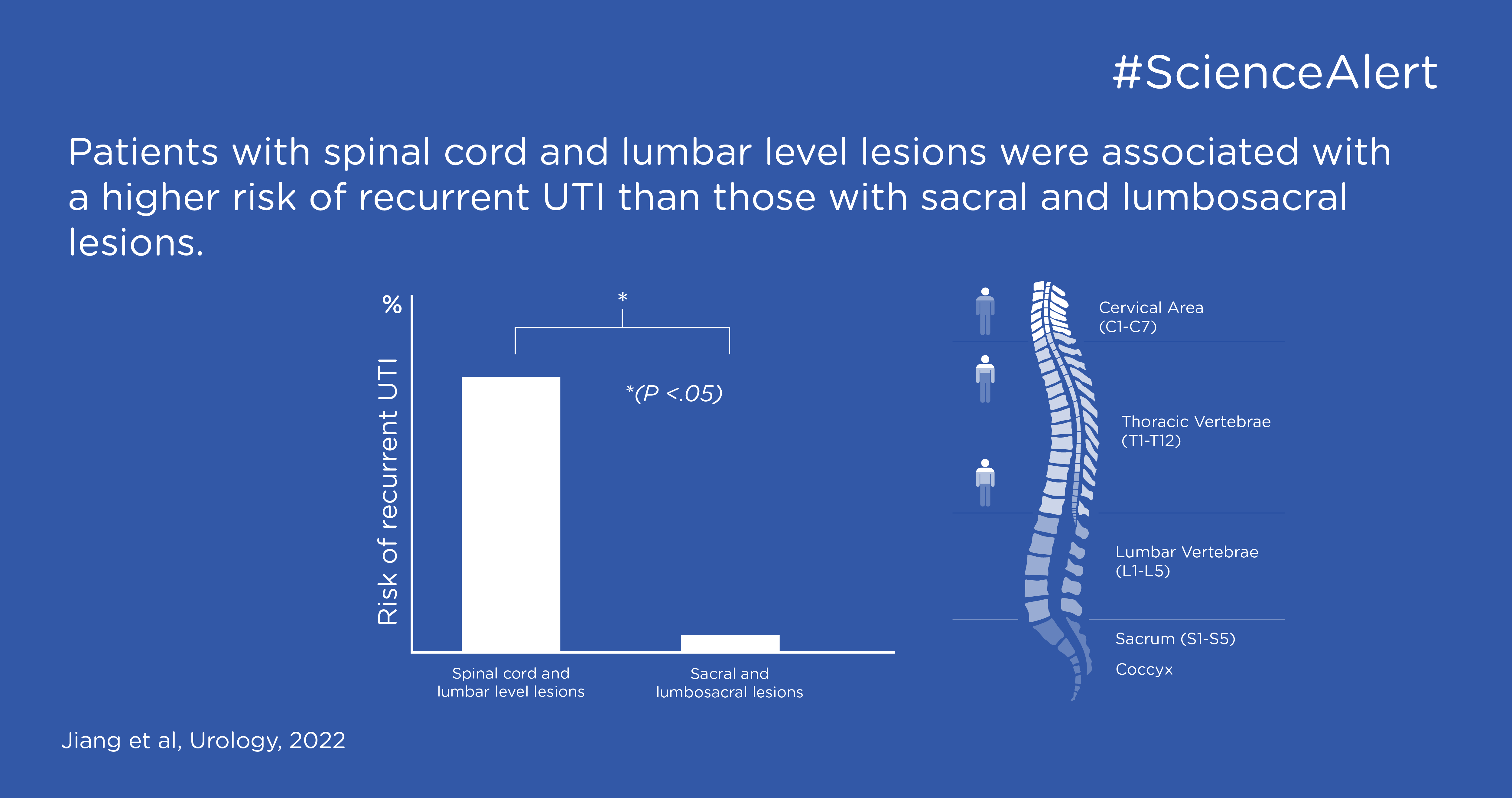
There are contradictory statements on how the level of injury affects the causes of UTIs. This study reported high-level spinal cord injury to be associated to a higher risk of recurrent UTIs. A higher spinal cord injury is more harmful to muscle function, which might lead to the possibility of VUR and lower bladder compliance.
Children with NB are at risk for Vesicoureteral reflux (VUR) due to the increase in bladder pressure, which overcomes the natural resistance of the ureterovesical junction and allows urine to flow in the wrong direction. The prevalence of VUR among children with recurrent UTI ranges from 20% to 50%. In adults it’s less frequent.
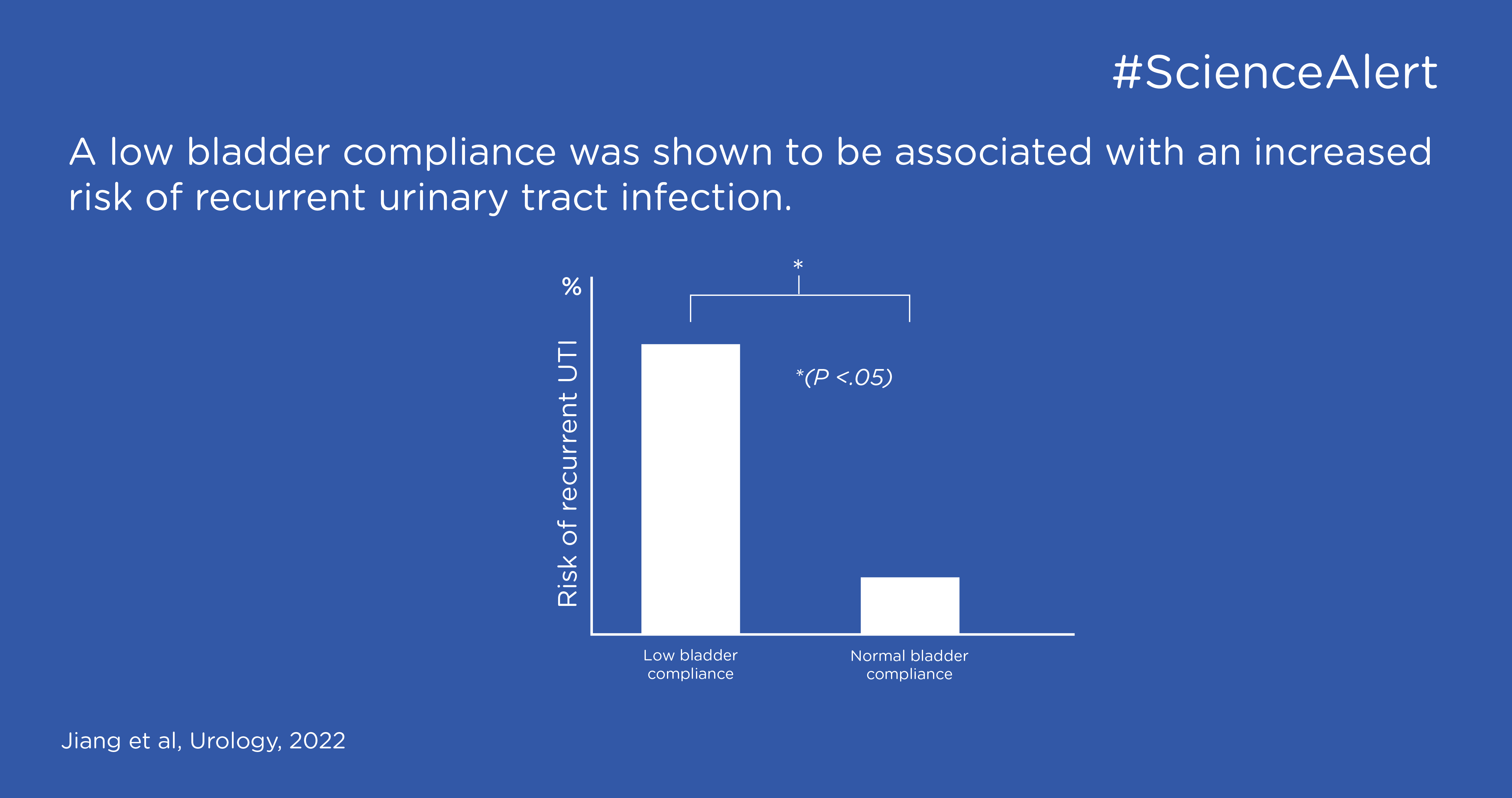
The study showed that bladder wall thickness (BWT) was a significant factor for the incidence of recurrent UTI, where a thicker bladder wall (mm) was associated with higher risk of recurrent UTI. Furthermore, it was shown that low bladder compliance (<10.0) was associated with an increased risk of recurrent UTI. Bladder compliance describes the relationship between change in bladder volume and change in detrusor pressure. This is generally regarded as a measure of bladder distensibility and is the key determinant regarding the patient’s risk for upper urinary tract impairment.
Previous studies have shown an increased risk of recurrent UTIs in people with constipation, however Jiang et al did not find a correlation between poor bowel management, and associated incomplete bladder emptying, and recurrent UTIs. Worth mentioning that 46% of the children in the study had constipation. Similarly, no association was found between the frequency of IC and risk of recurrent UTIs.
How to Prevent UTIs in Children
This study has identified a couple of risk factors for recurrent UTIs in children with neurogenic bladder which should be kept under special attention (older age, high level of spinal cord lesion, long duration of NB, presence of VUR, increased BWT, and low bladder compliance). Continuous antibiotic prophylaxis (small doses over a long time) did not seem to reduce the UTIs, and it is not recommended for the prevention of UTIs in this patient group. Every 6 months to 1 year it is recommended to follow up children with the demonstrated risk factors to avoid recurrent UTIs and severe kidney complications. To achieve this, regular clinical and urodynamic examinations are important.